Sever’s Disease: A common and treatable overuse injury
Sever’s disease is one of the most common causes of heel pain in growing children and teenagers (1).
It is named after James Warren Sever, an American doctor who first described the condition back in 1912. The condition refers to an inflammation of the growth plate in the heel, which can set in when this area is exposed to repetitive pressure, as a result of high impact activity (8).
We know that 6 % of all children between 7-14 years will develop Sever’s disease.
Heel pain caused by Sever’s disease can be relieved by our Solemaids Severs insoles. Last year 2500 children could stay active with Solemaids Severs in their shoes. From clinical data, collected since 2017, we know that 90 % have immediate pain relief with Solemaids Severs. The Solemaids Severs insoles were are developed in Denmark, by physiotherapist Per Øllgaard
What causes Sever's disease?
Sever’s disease is caused by repetitive stress to the growth plate of the heel bone in growing children and adolescents. During growth spurts, the growth plate area is particularly sensitive to pressure as it has not yet developed into solid bone.
If the heel bone is exposed to repetitive stress – for example from running, jumping and other high-impact activities – an inflammation can develop, which leads to swelling and pain. A research study show that most children experience pain in both heels (7).
Who get's Sever's disease?

Boys vs. girls
Boys are more prone to developing Sever’s disease than girls (3). We believe this is because of a steeper growth curve in boys than girls, which means that the body grows more in a shorter time, which also affects the heel bone. Boys between 11-14 years who play football are especially at risk of developing heel pain. This can also be because of Astro turf and football cleats that have no shock absorption, leaving the growing heel bone more vulnerable.
Age
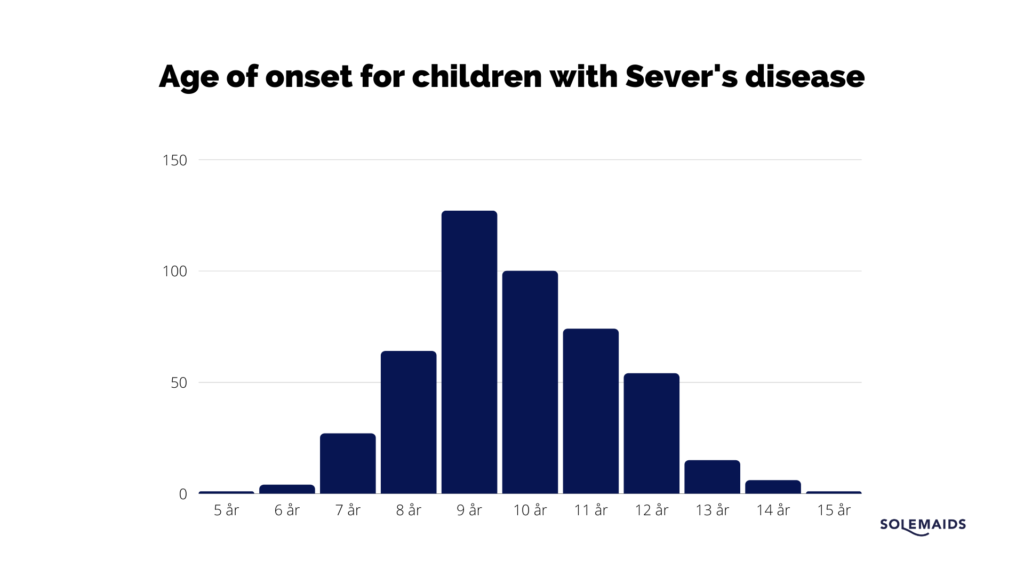
Sever’s disease is typically seen in children between the ages of 7 and 14. It can, however, set in earlier or later. The youngest case of Sever’s disease that physiotherapist, Per Øllgaard, has ever seen was a girl, 4 years old and the oldest was a boy, 17 years old. But most children are between 9-11 years old when Sever’s disease sets in (see table below). Usually, the growth zone in the heel closes at around 15 years, and the condition wears off.
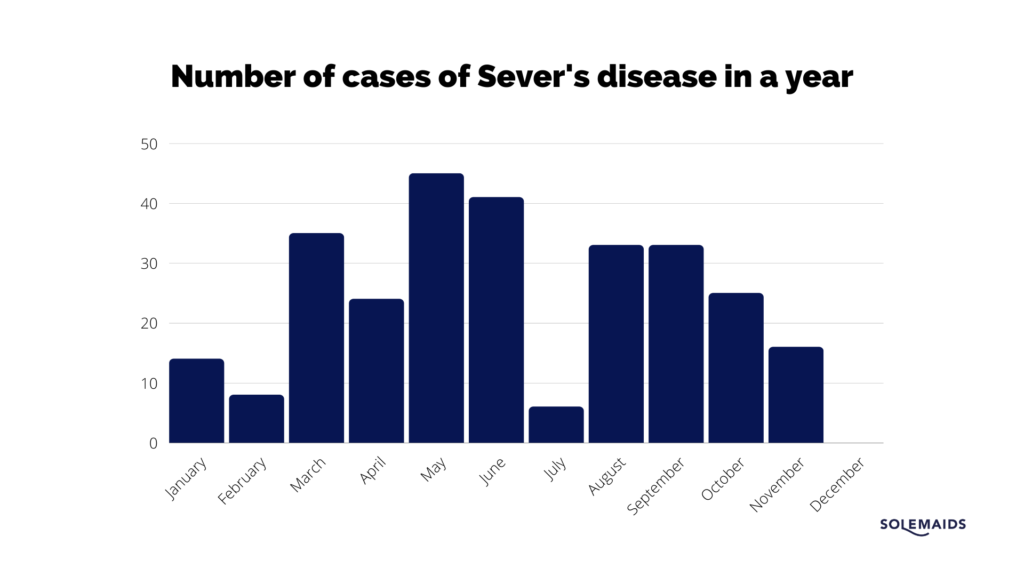
When do children get Sever’s disease?
Cases of Sever’s disease often peaks around spring and early autumn as this is when the sporting seasons are commenced (3). At Per Øllgaard’s clinic in Viborg, there were more cases of Sever’s disease in spring and autumn of 2021 (see table below). There were most cases in May where the children have been doing sports for some months and can no longer ignore their heel pain. The faster they can get help, the faster they can have pain relief.
Prevalence of Sever’s disease
A Danish study shows that Sever’s disease is the most common overuse injury among school children aged 8-14. Based on the number of children from the 10 schools within the age group and on the number of Sever’s disease diagnoses, it is estimated that 6 % of all children will develop Sever’s disease at some point for a shorter or longer period (6).
Children who are physically active or engaged in sports that involve a lot of running or jumping, especially on hard surfaces, have a greater risk of developing Sever’s disease (5, 1). In a Japanese study they investigated how many children on football teams suffer from Sever’s disease. The results were that up to 20% of the football players suffered from heel pain (9). This shows that the prevalence is higher among sports active children than in the regular population.
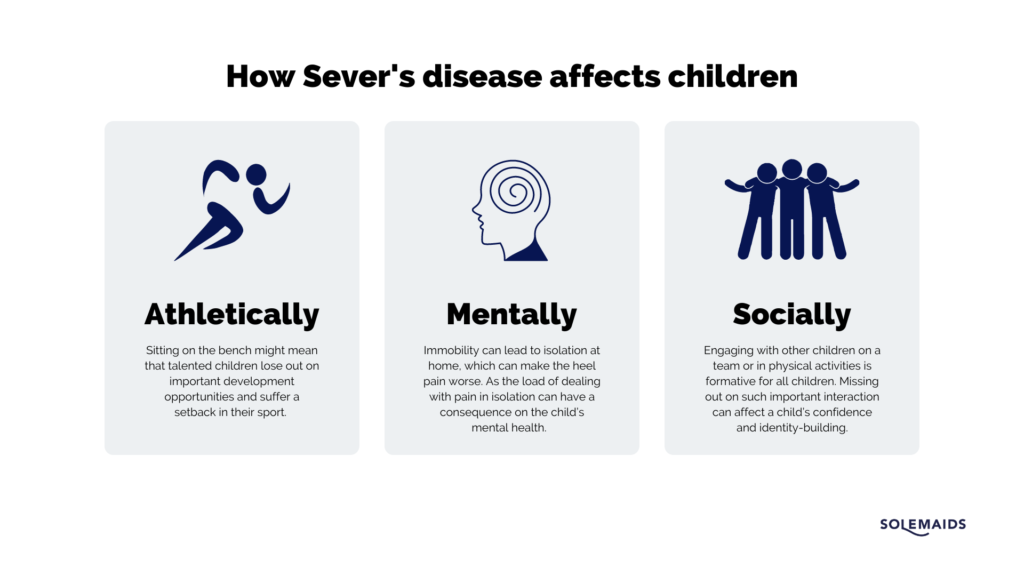
How does Sever’s disease affect children?
Children who suffer from Sever’s disease are affected differently, but research shows that it has a negative impact on children’s physical and social well-being and school life, which then has a significant impact on the health-related quality of life for these children (7).
Most children are told that the condition will pass as they get older and that they should rest when there’s pain. But this doesn’t help the children remain active, continue with their sport or play with their friends at school.
Therefore, telling an active child to be passive is unfortunate for several reasons.
Clinical experience shows that Sever’s disease is not cured by resting; it goes away as the child grows older. Reducing physical activity to a minimum will put a temporary end to the heel pain. As soon as the child resumes their activity, the pain typically returns.
From our own data collection in 2021 we know that most children have had pain for 10,8 months in average, meaning that some children push their pain away and hide it until they cannot do it anymore.
How to diagnose for Sever’s disease?
Sever’s disease is an underdiagnosed overuse injury, as a lot of health professionals don’t know enough about it or anything about it at all.
If a child complains of heel pain, it’s nearly always Sever’s disease as almost no other diagnoses exist. From some studies on the prevalence of Sever’s disease, we can see that all heel pain complaints are not diagnosed as Sever’s disease. From 226 heel findings only 49 children are diagnosed with Sever’s disease. These diagnoses have been given primarily due to radiographic or ultrasonic examination (9). As other diagnoses for children’s heel pain are rare, it seems to us that these other heel findings are most likely also Sever’s disease. An Australian study looking into the development of the heel bone in children, also suggests that all heel related pain in children should be diagnosed and treated as Sever’s disease (2).
Physical examination and interview is sufficient to diagnose Sever’s disease
Many studies also find that anamnesis and physical examination are sufficient for correct diagnosis (3) and with a simple set of tests (link), a positive squeeze test is a clear indicator for Sever’s disease (5). Another study also concludes that the diagnosis should be made primarily by anamnesis and physical examination, thus reducing the “Number of radiographs needed, and therefore minimise exposure to radiation in paediatric patients.” (2)
How to test your child for Sever’s disease
Are you not sure if heel pain is caused by Sever’s disease? Can you tick off the following boxes?
If so, it is likely that your child suffers from Sever’s disease and can be helped with our Solemaids Severs insoles.
There are two ways to test your child for Sever’s disease:
- The squeeze test
- The heel-walking test
Watch the video to see how you perform these two tests.
The levels of Sever’s disease
In Solemaids we work with our own categorization for different levels of Sever’s disease. If your child is in level 2, 3, or 4, we recommend that you contact a Solemaids specialist near you.
Level 1: Experiences heel pain after physical activity
Level 2: Experiences heel pain during and after physical activity
Level 3: Takes breaks during physical activity or can only participate with limited movement due to heel pain
Level 4: No longer participates in physical activities due to heel pain
Recovery from Sever’s disease
According to a German study, Sever’s disease is categorised as either a moderate or severe injury as recovery takes more than 4 weeks (1). At a youth football academy in Germany, they found that it can take several months for patients to be pain-free even after getting the diagnosis and beginning treatment. It took the players on average 4 weeks to return-to-play after commencing treatment (1). This shows treating heel pain with rest, ice and exercises are not sufficient as recovery-time is too long.
Therefore, we in Solemaids have a task to bring information to parents and coaches about the Solemaids Severs insoles that can help children almost immediately and have them return to play much faster.
How to treat Sever’s disease?
Many studies suggest and find that using multiple treatments can relieve pain. This includes strengthening, stretches, ice, rest, orthoses and anti-inflammatory drugs. In Solemaids we don’t believe it to be that complicated. From experience, we know that for children, the more you have to do, to relieve pain, the worse the child might find themselves to be. It’s not recommended to use drugs and painkillers on children.
A simple insole solution with Solemaids Severs relieves pain immediately in 90 % of all children. Treating children’s heel pain is not about removing the injury or relieving pain completely. What matters is to get a significant pain relief, so the child can remain active and participate in sports. It’s not the child that needs a break, it’s the heel! The most important thing when treating children with Sever’s disease is to not immobilise them, but to let them stay active!
What research says about treatment for Sever’s disease
There are not enough studies to have a best practice for treating Sever’s disease in children (7). Treatment regimens are then often based on similar studies for heel pain or Achilles tendon overuse injuries among adults (4). The few studies that investigate this agree that there is something to do for Sever’s disease and that the main goal should be “pain relief” and “a return to sports and physical activity with full recovery.” (5)
Most common traditional treatments for Sever’s disease include stretching and strengthening exercises, rest, icing, heel lifts, heel cups, anti-inflammatory drugs and pain reducing medicine, even though these have not been evaluated properly (4).
“The literature suggests that, with proper intervention, most patients with Sever’s disease are able to return to sports within a few weeks to two months… Furthermore, one study stated that, on rare occasions, it has taken up to six months to recover from Sever’s disease, whereas others have reported that, in some cases, the pain could continue until growth ceases.” (4)
The question we then believe we should all ask is if it’s good enough that some children are in pain and inactive for several months? We don’t think so. That’s why we have developed the Solemaids Severs insoles that in 90 % of cases gives children immediate pain relief.
References
Belikan, Patrick, Lars‑Christopher Färber, Frédéric Abel, Tobias E. Nowak, Philipp Drees and Stefan G. Mattyasovszky. 2022. Incidence of calcaneal apophysitis (Sever’s disease) and return-to-play in adolescent athletes of a German youth soccer academy: a retrospective study of 10 years, Journal of Orthopaedic Surgery and Research, no. 17, vol. 83. Pp. 1-6.
Blythe, Connor S., Mikaela S. Reynolds and Laura S. Gregory. 2022. Quantifying the ossification and fusion of the calcaneal apophysis using computed tomography, Journal of Anatomy, pp.1-16.
Ceylan, H. H. and Caypinar B. 2018. Incidence of calcaneal apophysitis in Northwest Istanbul, Musculoskeletal Disorders, 19:267. Pp. 1-5.
Elengard, Thomas, Jón Karlsson and Karin Grävare Silbernagel. 2010. Aspects of treatment for posterior heel pain in young athletes, Open Access Journal of Sports Medicine, no. 1. Pp. 223-232.
Fares, Mohamad Y., Hamza A. Salhab, Hussein H. Khachfe, Jawad Fares, Rachid Haidar and Umayya Musharrafieh. 2021. Sever’s Disease of the Pediatric Population: Clinical, Pathologic, and Therapeutic Considerations, Clinical Medicine & Research, vol. 19, no. 3. Pp. 132-137.
Fuglkjaer S, Hartvigsen J, Wedderkopp N, Boyle E, Jespersen E, Junge T, Larsen LR, Hestbaek L. 2017. Musculoskeletal extremity pain in Danish school children – how often and for how long? The CHAMPS study-DK, BMC Musculoskelet Disord, 18(1):492.
James, Alicia M., Cylie M. Williams and Terry P. Haines. 2016. Health related quality of life of children with calcaneal apophysitis: child and parent perceptions, Health and Quality of Life Outcomes, 14:95. Pp. 1-7.
Sever, J. 1912. Apophysis of os calcis, NY State Journal of Medicine, vol. 95, no. 1025.
Suzue, Naoto, Tetsuya Matsuura, Toshiyuki Iwame, Daisucke Hamada, Tomohiro Goto, Yoichiro Takata, Takenobu Iwase and Koichi Sairyo. 2014. Prevalence of childhood and adolescent soccer-related overuse injuries, The Journal of Medical Investigation, vol. 61. Pp. 369-373.
Øllgaard, Per and Birgitte Folmann. 2017. Sever’s Disease – overlooked and painful, but treatable. Discriptive study at Per Øllgaard Fysioterapi, Viborg.